If a picture is worth a thousand words, what’s the value of a neuroradiology image of a brain contusion? If it helps to prove the existence of a head injury in your car accident case, it could be worth a great deal in compensation from the at-fault driver’s insurance company. A good personal injury attorney must be aware of the different neuroradiology images available and what they mean, as well as how and when to use them.
Computed Tomography (CT) Scans
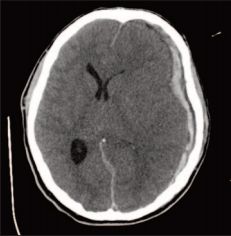
A CT Scan does not show a mild traumatic brain injury (mTBI) or concussion. A CT Scan is useful for more moderate to severe forms of brain injury. It can show bleeds; fractures; ventricle displacement, loss, and enlargement; or midline shift, etc. For example, below is a CT Scan image for a young man who sustained Second Impact Syndrome in a high school football game after being prematurely returned to play. Here you can see a sub dural hematoma, a midline shift, and ventricle displacement, loss, and enlargement.
Magnetic Resonance Imaging (MRI)
With MRIs there are different weights, such as 1.5T, 2T, and 3T. These weights are the strengths of the magnets and the thinness or thickness of the slices, the higher the weight and the thinner the slice, the more likely it is that findings will appear on the MRI. The 3T MRI is optimal with higher resolution and thinner slices. This allows the neuroradiologist to find contusions and shearing that can be present with mTBI due to the enhanced detection capabilities. For example, below is a 3T MRI with thinner slices where the neuroradiologist was able to detect a subtle interior temporal contusion.
Diffusion Tensor Imaging (DTI)
DTI is an MRI based neuro-imaging technique that enables measurement of the restricted diffusion of water flow along axons in the brain tissues and compares the diffusion to the axons in a white matter fiber tract. Axons can be thought of as the “telephone wires” of the brain. DTI provides a unique insight into the brain to measure the neural tract in comparison to a normative database to determine injured areas of the brain. This comparison yields a numerical value regarding the health of the axons. Low values are indicative of axonal injury. In addition, the DTI findings can be matched to the area of injury shown on other imaging, such as MRI. Physical findings that are consistent on more than one type of imaging is objective proof of brain injury. Below is an example where the DTI matched shearing (tearing) as seen on an MRI.
“Despite significant variability in sample characteristics, technical aspects of imaging, and analysis approaches, the consensus is that DTI effectively differentiates patients with TBI and controls, regardless of the severity and timeframe following injury. Furthermore, many have established relationship between DTI measures and TBI outcomes.”2
NeuroQuant
NeuroQuant measures the volume of structures of the brain and compares that information to existing reference data gathered from “normal” brain measurements, adjusted for various factors such as cranial capacity, age and sex, to assist with diagnosis of neurological conditions, including traumatic brain injury. Initial testing can be done as part of a traditional MRI procedure after an injury and compared to follow-up testing later to help measure the differences for brain atrophy or other brain damage. In particular, NeuroQuant can be a very effective tool to show traumatic brain injury resulting from carbon monoxide exposure. Carbon monoxide exposure causes diffuse brain injury, meaning multiple lobes throughout the brain lose volume (injury) as opposed to a focal injury in a specific location, such as when the front and back portions of the brain are injured during a whiplash-type mechanism of injury. Measured loss of volume in the lobes diffusely throughout the brain can objectively prove that a person suffered a brain injury as a result of carbon monoxide exposure. Below are photographs showing global atrophy in the form of abnormal ventricular volume.
Susceptibility Weighted Imaging (SWI) and Gradient Echo (GRE)
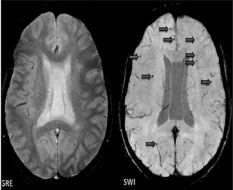
SWI and GRE are two additional tools for objectively showing brain injury. These tools allow the neuroradiologist to detect microhemorrhages (tiny bleeds in the brain) and calcifications. SWI uses a slightly different sequence and is 4-6 times more likely to find hemorrhages than its GRE counterpart, see the below comparison:
Clinical Correlation Required
In consideration of all the various types of imaging that can be used to prove a brain injury, the findings that are most likely related to trauma include atrophy of the brain (global, hippocampal, cortical); white matter shearing and hyper intensities; bleeding, sudden swelling, and structural damage; and positive DTI findings. However, these findings mean nothing unless there is clinical correlation. This means that the positive finding on imaging needs to be clinically correlated by a medical professional both to the mechanism of injury as well as the clinical presentation of symptoms. Factors to consider as part of the clinical correlation include age, the mechanism of injury, any history of trauma or clinical suspicion, positive additional findings on imaging scans, exclusion of other risk factors, and the size and number of deviations from normal.
If You Can’t See It, Does it Exist?
Certain defenses are commonly brought in traumatic brain injury cases to argue against the existence of the brain injury itself and question whether the injured person experienced and continues to experience symptoms from the brain injury. One such argument in brain injury cases emerges when a CT Scan shows no abnormal findings. This may be offered as proof that a person did not suffer a brain injury. As illustrated above, however, CT Scans do not show concussions or mTBIs. This underscores the importance of retaining a personal injury lawyer who is knowledgeable about the various neuroradiology images available for diagnosis of a fuller range of brain injuries.
Finally, it is equally important to remember that, although other types of imaging exist to detect microhemorrhages and other small abnormalities in the brain, not all TBIs will be visible regardless of the type of imaging used. Does this mean the brain injury doesn’t exist? The answer is no. Medical providers treat symptoms, not imaging.
Christopher A. Mutch, et al., Imaging Evaluation of Acute Traumatic Brain Injury, 27 NEUROSURG. CLIN. OF N. AM. 409-39 (2016), available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5027071/.
M.B. Hulkower, et al., A decade of DTI in traumatic brain injury: 10 years and 100 articles later, 34 AM. J. NEURO – RADIOL. 2064-2074 (2013), available at http://www.ajnr.org/content/34/11/2064.
Eric R. Braverman, et al., Evoked Potentials and Memory/Cognition Tests Validate Brain Atrophy as Measured by 3T MRI (NeuroQuant) in Cognitively Impaired Patients, 10 PLOS ONE 8 0133609 (Aug. 5, 2015) available at 10.1371/journal.pone.0133609.